

In children with sickle cell disease (SCD), cerebral vasculopathy is responsible for overt strokes and silent cerebral infarcts (SCI). Transcranial Doppler (TCD) detects children at risk of strokes (intracranial time averaged mean of velocities (TAMV) ≥200cm/s). The extracranial portion of the internal carotid artery (eICA) can also be the site of stenosis or occlusion. eICA assessment requires cervical Doppler using a submandibular approach and cervical MRA (cMRA). We previously reported that eICA TAMV≥160cm/s are highly predictive of eICA stenosis and are a risk factor for SCI independently of acute and chronic anemia. However, the kinetics of eICA arteriopathy are unknown. The aim here was to evaluate and compare the cumulative incidence of intra/extracranial arteriopathy and associated risk factors in a longitudinal SCD cohort.
Children born between 01/1988 and 01/ 2018, followed at our center at least until 06/2012 and up to 09/2019, annually assessed by TCD imaging and at least once by cervical Doppler were included, resulting in 493 SCD children (238F-255M) with 398 SCA (385SS,10Sb0,3SDPunjab), and 95 SC/Sb+ children (65SC,30Sb+). Alpha-genes, b-globin haplotypes, G6PD activity, CD36 expression were recorded. The average of baseline biologic parameters recorded between 1 and 3 years of age, a minimum of 3 months away from transfusion, 1 month from a painful episode, and before any intensive therapy was calculated. The median (range) follow-up of the overall cohort was 10.6 years (1.1-22.9), providing 5335 patient-years of follow-up. Six deaths occurred (5 SCA-children at 2, 4, 7, 19 & 20 years and 1 in SB+ patient at 13 years). Three SS patients had an ischemic stroke at 1.5, 3 and 4.3 years.
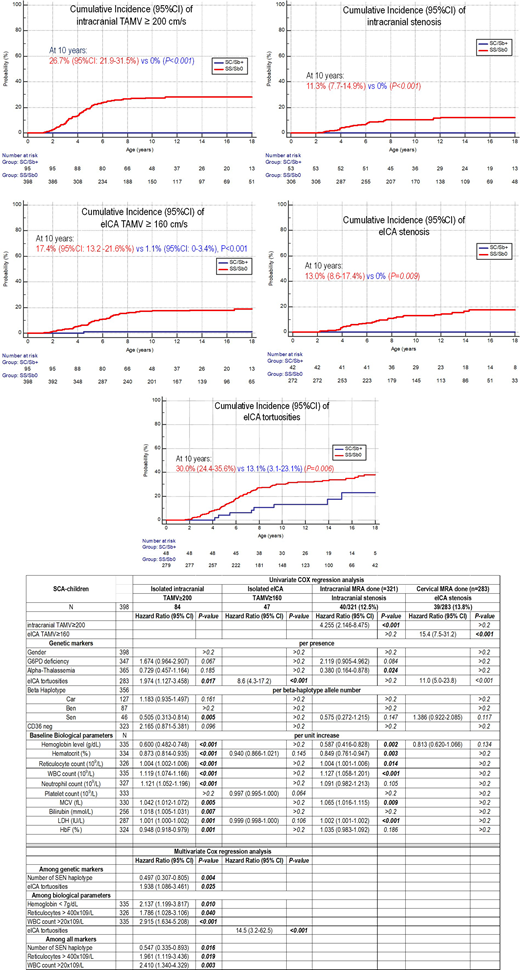
Kaplan-Meier estimates of cumulative incidence (95%CI) are shown (Figure). In SCA-children, abnormal eICA TAMV and/or eICA stenosis were sometimes associated with abnormal intracranial TAMV and/or stenosis, but isolated eICA TAMV≥200cm/s or 160-199cm/s were observed in 19 (4.8%) and 28/398 (7.0%) patients, respectively, and isolated eICA stenoses in 33/294 (11.2%).Thus, risk factors were only analyzed in patients with isolated intra- or extracranial arteriopathy. COX regression analyses are shown (Table).
For isolated intracranial TAMV≥200cm/s, multivariate analyses after introducing all significant genetic and biological risk factors retained the number of SEN b-haplotypes [HR=0.547 (95%CI:0.335-0.893); p=0.016], reticulocyte count>400x109/L [HR=1.961 (95%CI:1.119-3.436); p=0.019], and WBC count>20x109/L [HR=2.410 (95%CI:1.340-4.329); p=0.003] as independent risk factors.
Isolated eICA TAMV≥160 cm/s were only strongly associated with the presence of tortuosities [HR=8.6 (95%CI :4.3-17.2); p<0.001]. eICA tortuosities were present in 94/284 (33.1%) SCA vs 5/43 (11.6%) SC/Sb+ children (p=0.004), most often seen at the first cMRA but secondarily in 16 patients. Multivariate COX analysis retained genotype [HR/SCA vs SC/Sb+ = 3.6 (95%CI:1.4-9.4); p=0.010], low hemoglobin [HR=1.25 (95%CI:1.04-1.50); p=0.020], and high LDH [HR=1.002 (95%CI:1.001-1.002); p=0.001], as independent risk factors for eICA tortuosities.
As expected, the risk of intracranial stenosis was significantly associated with isolated intracranial TAMV≥200 cm/s [HR (95%CI)=4 .255 (2.146-8.475); p<0.001]. After adjustment with isolated intracranial TAMV≥200 cm/s, a-thalassemia, low hemoglobin, high WBC, MCV and LDH remained as significant, but not independent, risk factors for intracranial stenosis.
The risk for eICA stenosis was only highly associated with the presence of tortuosities [HR=10.9 (95%CI:4.7-25.0); p<0.001], or a history of eICA≥160cm/s [HR=15.4 (95%CI :7.5-31.2); p<0.001].
This study reports eICA arteriopathy kinetics using a longitudinal cohort of SCD children systematically assessed by Doppler and cMRA. While we confirm that only SCA and not SC/Sb+ children are at risk of intra/extracranial arteriopathy, we show for the first time that extracranial arteriopathy progressively develops as early as 2 years old in SCA-children and reaches a plateau around 10 years of age, as for intracranial arteriopathy. Furthermore, eICA tortuosities, which are the risk factor for eICA arteriopathy, are themselves significantly and independently associated with the SCA genotype and the severity of hemolytic anemia.
Bernaudin:BlueBirdBio: Consultancy; AddMedica: Honoraria, Other; GBT: Membership on an entity's Board of Directors or advisory committees. Verlhac:BlueBirdBio: Consultancy; AddMedica: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal